- by foxnews
- 23 May 2025
‘A gamechanger’: this simple device could help fight the war on abortion rights in the US
‘A gamechanger’: this simple device could help fight the war on abortion rights in the US
- by theguardian
- 22 Apr 2023
- in politics

1.9 k views
Joan Fleischman has always had people flying in from across the world to her private abortion practice in Manhattan. In the two decades her clinic has been open, she has seen clients from places such as Ireland, the Bahamas and Mexico, who couldn't get abortions in their home countries. In the past year, that has changed. Since the US federal right to abortion was overturned in June last year, she is now more likely to see patients flying in from her own country.
Often they are from Texas, sometimes Ohio, or Florida. Some with links to the city, others with none.
After years of providing abortion care, Fleischman, 60, still finds these trips shocking. "Usually, if somebody needs unusual medical care, they are willing to fly around the world for it - like for advanced neurosurgery or something. It's always struck me as incredible that people are flying to me for the most simple procedure."
There's a reason people fly to see Fleischman. She provides abortions through manual uterine aspiration - using a small, hand-held device to remove pregnancy tissue. The device is gentle enough that the tissue often comes out almost completely intact. It is a quick and discreet procedure where a patient might be in and out of the door in less than an hour.
Fleischman is a co-founder of the MYA Network, a network of primary care clinics and clinicians in 16 states. They believe the tool could be radical in the hands of more primary care clinicians - clinicians they are amping up to train.
The time to do that, they say, is now. The future of mifepristone, a major abortion pill used in more than half the abortions in the US, is in question due to a lawsuit brought by anti-abortion groups seeking to overturn the FDA's approval of the drug. It could be determined by the same supreme court that ruled last year to overturn Roe v Wade.
Manual aspiration is not new: it is used by many big abortion clinics across the US. But those are notoriously overstretched. In 2020, before Roe v Wade was overturned, 38% of reproductive-age women lived in counties with no abortion provider at all.
Especially given the threat to mifepristone, the MYA Network believes primary-care clinicians, who are vastly more common than abortion providers, are well placed to help.
But while more than 73% of primary-care doctors believe abortion care to be within their scope of practice, a tiny fraction - less than 10% - of primary-care doctors actually provide it.
The network is planning to unveil an online curriculum and in-person trainings for the procedure, which many of the clinicians and institutions in the network have already been doing in their own states.
"The number of clinicians who could be trained would be limitless," says Michele Gomez, a co-founder of the MYA Network of clinicians.
"There are so many clinicians out there who want to do something to help but just don't know how, and this information and support could be a gamechanger."
As a young woman, Fleischman often felt compromised. She frequently traveled overseas as a teenager to do basic aid work with a volunteer group, and would feel fear and humiliation from the unwanted sexual attention she would receive. That was the beginning of her understanding, as she describes it, of the constant vulnerability women walk around with.
By 18, Fleischman had had her first abortion - an experience she describes as routine, mundane even. The pregnancy came as she started her first year at the University of Chicago, and was the least of her concerns. "It was a no-brainer. I was like, 'Pregnant? Nope, I'm going to be a doctor.' So I went to Planned Parenthood and took care of it," says Fleischman.
It wasn't until she started providing abortions that she even thought about the experience again.
Fleischman was in her 30s, living in New York and already trained as a family practice doctor, when she saw an advertisement offering to teach doctors how to do surgical abortions.
"I realized that after all these years in training, I'd never got to even see an abortion. I had saved lives, helped people at the height of the Aids crisis. I had delivered babies. These are things a family doctor does," she says. "I was like, 'Why? That's ridiculous.' That's where the passion started."
Fleischman took up more training, learning to perform abortions at a Planned Parenthood, in 1995.
Planned Parenthood - as Fleischman pointed out herself - is the place where people "go to get it done". It is a vital lifeline for many people, providing hundreds of thousands of abortions every year, many to low-income and uninsured clients.
But the efficiency of their service contrasted with Fleischman's training as a family doctor - which emphasizes the importance of the doctor-patient relationship. She was used to that relationship entailing a level of intimacy - her work involved home visits with patients, and entering lifelong relationships with them and their families.
Fleischman recalls her Planned Parenthood training: "Women went station to station. They got their blood drawn, and then they sat in a little waiting room with other people. They got their ultrasound; they sat in another little waiting room, always with paper gowns on. They had been fasting for the whole night before. They saw a counsellor. Then they were in a bigger waiting room. And then they got called by name, to come in for their procedure. The surgeon went from room to room to room, doing 50 to 60 abortions a day."
She wanted to personalize the experience. For patients to be able to come in with their partners, to be talked through their options and their concerns, fully. "I just felt so disconnected. It seemed to me that the doctor was really a technician emptying uteruses," she continues.
"I was like, 'I want to create a different model. I want people to have a different experience going through this'."
As the US is learning, ethical quandaries always arise when abortion is banned: what to do for the woman who turns up septic after a failed self-managed abortion? How to deal with life-threatening pregnancies that require intervention but also require an abortion? What about cases of rape, incest or pregnant children?
Essentially: how much pain is the state willing to impose on people when it restricts reproductive freedom?
In Bangladesh, a sort of answer to some of these questions came following the 1971 civil war, during which soldiers abducted Hindu and Bihari Muslim women and set up rape camps. Pregnancy as a result of rape rocketed; in the following years, suicide and maternal mortality also shot up. Abortions, of course, did not stop happening. In 1978, while abortion remained illegal, an estimated 800,000 abortions took place in the country, resulting in about 8,000 deaths.
"Menstrual regulation", as it came to be known - using the same manual aspiration technique that Fleischman now uses - became a sort of legal loophole, allowing safe abortions for early pregnancies.
By 1974, menstrual regulation was legal and by 1979, Bangladesh started providing the procedure through its national family planning program.
Now, one might walk through a busy street in Bangladesh and find a sign advertising menstrual regulation in a country where, at least officially, abortion is only allowed in life-threatening situations. A woman simply comes in and explains she has missed her period. She doesn't take a pregnancy test before the procedure, and nobody asks her to. As long as she sees the clinician before 12 weeks, they will "restore her period" for her.
"It's just a clever policy, a wink and a nod - everybody knows what's going on. It's kind of a recognition that women need this care," says Bill Powell, a senior medical scientist at IPAS, an international organization that trains medical professionals across the world to use manual aspiration.
It also gives doctors discretion without explicitly violating the law.
"They say: 'I know if I don't provide this care, this woman is going to go off and do something that is unsafe, and she'll be back to my facility ill, needing emergency care, so therefore, I am saving her life by providing this procedure,'" Powell explains.
Fleischman, who worked in Bangladesh in her youth, and her colleagues in the MYA Network are adamant they are only proposing manual aspiration be used legally in the US - for abortion care where it is legal, and miscarriage management where it is not. But its use in ordinary medical settings could still provide a radical opportunity in the US, she says, by expanding the number of clinicians who can easily perform the procedure up until 12 weeks.
Others have touted this idea, in a slightly different way: anyone can learn to use a manual aspiration device, and manage their own abortions, some activists argue. All they need to learn to do is to insert a cannula, which is like a large straw, through the natural opening of the cervix, and then attach the aspiration device. The device is like a syringe, which creates a vacuum. Once the pressure is released, the contents of the uterus are gently removed. The self-management option has other advantages - like cutting out the middle man in a climate where doctors are increasingly scared to provide abortion care, and equipping people with self-knowledge when the future of access to abortion is unclear.
Fleischman understands the necessity of self-managed abortion, especially in places where the procedure is illegal. But she believes that after receiving care, people should always be able to follow up with a clinician who knows their case if anything goes wrong, or even if it doesn't. It dismays her that people are living in a climate in the US where they might not have that option; where people might be too scared to look for help; and where they may suffer with complications alone in the rare instances when something does go wrong.
In states where abortion is legal, manual aspiration provides the opportunity to treat abortion like mainstream medicine, rather than something that's siloed into abortion clinics, which are visible, small in number and under constant threat.
The case brought by anti-abortion groups against the FDA's approval of mifepristone - which is one of two abortion drugs used in more than half of all abortions in the US - will almost certainly be decided by the supreme court. The uncertainly over its future, Fleischman argues, could make the expanded use of manual aspiration critical to preserving abortion and miscarriage care.
Some providers may switch to abortions using only the second drug, misoprostol. But misoprostol-only abortions are slightly less effective, and more often require care for incomplete abortions. That could result in straining already stretched abortion clinics, which will probably have more people knocking at their doors for both surgical abortions and follow-up care.
With manual aspiration on the other hand, doctors can be mostly certain that the procedure is complete before the patient leaves the state.
Bennett trains several dozen students a year in manual aspiration, teaching them the procedure as part of their regular medical training, and says students are actively seeking out this instruction in the new, post-Roe environment.
Students "are selecting programmes where abortion care is integrated into their training, even over some that might be more prestigious", he says.
Clinicians in areas that border states with bans, which have seen big increases in demand for abortion services as a result, are also a target for training, as are "red parts of blue states", explains Gomez.
Clinicians in states where abortion is legal who want to do something to fight the war on abortion could easily do so by integrating abortion into their practices, Fleischman and her colleagues say.
"It's done in a couple of minutes," explains Fleischman.
"When it's done, you know that it's done. There's very few bleeding issues. You walk into an office, and an hour later, it's resolved. I have people flying in and out from Dubai for this procedure. They schedule the appointment, they come in, and they depart that afternoon," she continues.
"There's absolutely no reason this shouldn't just be part of regular medicine."
you may also like


- by foxnews
- 23 May 2025
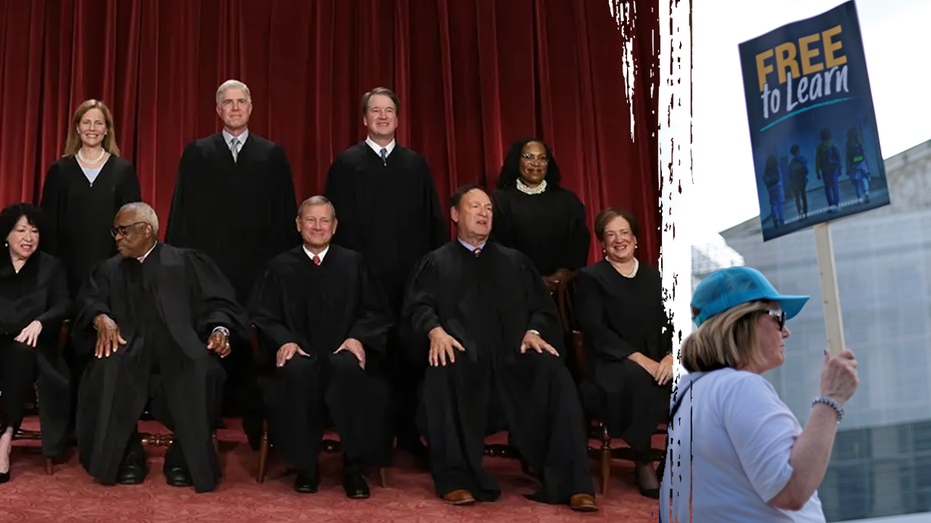
Supreme Court upholds Oklahoma decision, in blow to religious charter schools



travel
- by foxnews
- descember 09, 2016
United Airlines flight returns to Hawaii after concerning message found on bathroom mirror; FBI investigating
United Airlines Flight 1169 to Los Angeles returned to Hawaii after a "potential security concern" aboard the plane. The FBI and police are investigating.
read more